Medical decision making is the cognitive process clinicians use to gather, evaluate, and apply clinical information to reach diagnostic and treatment choices that best serve patient health goals. As a discipline, it integrates decision psychology, health economics, and clinical epidemiology to move care beyond intuition toward evidence-based judgment. For healthcare professionals and students, understanding medical decision making is the foundation of sound clinical practice. Every diagnosis, every test order, and every treatment plan flows from this process.
What is medical decision making and why does it matter?
Medical decision making, also called clinical decision making, is defined as the structured process of reducing diagnostic uncertainty by integrating clinical data, patient values, and probability estimates to balance risks against benefits. The Merck Manual describes a practical example: when a diagnosis reaches 98% probability, the focus shifts from further testing to treatment utility. That single insight changes how you allocate time and resources at the bedside.
The importance of medical decision making extends beyond individual patient encounters. Poor decisions drive unnecessary testing, missed diagnoses, and preventable harm. The Society for Medical Decision Making recognizes the field as a formal discipline that uses statistical and modeling techniques to improve both clinical care and health policy. Understanding its principles gives you a framework that works across specialties and clinical settings.
What are the key components of the medical decision making process?
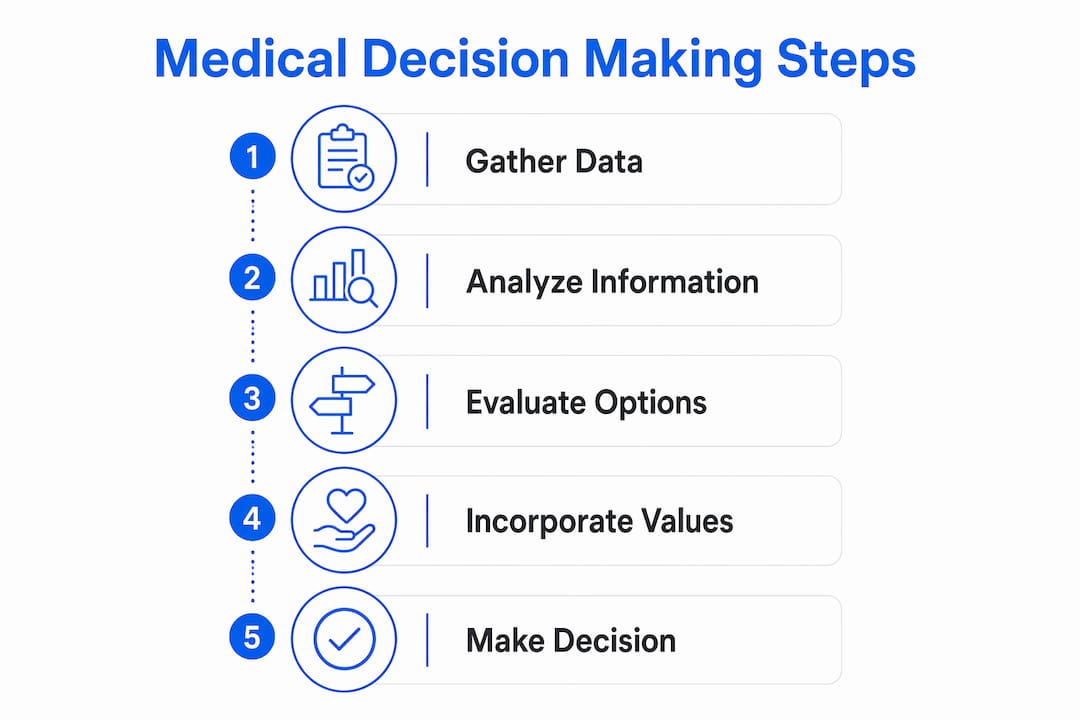
The medical decision making process moves through several cognitive stages. Each stage carries its own risks if skipped or rushed.
- Pattern recognition. Clinicians match a patient's presentation against stored mental templates from prior experience. This is fast and efficient for common, clear-cut cases.
- Hypothesis generation. When the pattern is ambiguous, you generate a differential diagnosis. You rank possibilities by probability and clinical urgency.
- Pre-test and post-test probability. Bayesian reasoning formalizes this step. You estimate the likelihood of a diagnosis before a test, then update that estimate based on the test result. A positive D-dimer in a low-probability pulmonary embolism patient carries different weight than in a high-probability patient.
- Clinical thresholds. The treatment threshold is the probability above which treatment proceeds without further testing. The testing threshold is the probability below which you can safely rule out a diagnosis without testing. These thresholds prevent both over-testing and under-treatment.
- Risk-benefit analysis. Every intervention carries potential harm. You weigh the probability of benefit against the probability of harm, factoring in the patient's specific circumstances.
Pro Tip: When a case feels straightforward, that feeling is your cue to pause. Pattern recognition is efficient but vulnerable to premature closure. Run a quick mental check: "What else could this be?" before committing to a diagnosis.
The analytical and intuitive modes are not opposites. Experienced clinicians switch between them deliberately, using pattern recognition for speed and Bayesian reasoning to confirm or challenge the initial impression. The skill is knowing when to shift gears.

How does shared decision making influence medical decisions?
Shared decision making is a collaborative process that combines clinical expertise with patient values to reach a treatment plan both parties understand and support. The American Academy of Family Physicians describes a structured model built on three conversations: team talk, options talk, and decision talk. Each conversation has a distinct purpose, and together they can be completed in about 2.5 minutes. That figure surprises most clinicians who assume the process takes far longer.
Shared decision making does not require the patient and clinician to reach full consensus. The goal is patient understanding and alignment with personal values, not agreement on every clinical detail. This distinction matters because it removes a major psychological barrier for busy clinicians.
Common barriers to shared decision making include:
- Time pressure. Structured models like team talk, options talk, decision talk address this directly by keeping each conversation focused.
- Clinician perception that patients resist involvement. Research shows this perception is often inaccurate. A clear invitation to participate and an assurance of support typically overcomes patient hesitation.
- Complexity of options. Presenting two or three concrete choices with plain-language risk descriptions reduces cognitive overload for patients.
- Documentation gaps. Failing to record the shared decision making conversation creates compliance and coding risk, particularly for complex visits.
Pro Tip: Frame the options talk around what matters to the patient, not what is medically optimal. Ask: "What are you most worried about?" That one question surfaces values that change the treatment plan more often than any lab result.
Aligning care plans with patient values also reduces non-adherence. A patient who understands why a medication was chosen and agrees with the reasoning is more likely to take it consistently.
What are common cognitive biases and challenges in clinical decision making?
Cognitive biases are the single largest source of diagnostic error in clinical practice. Premature closure, the tendency to stop considering alternatives once a plausible diagnosis appears, is the most common. Failure to switch from intuitive to analytical thinking causes clinicians to miss diagnoses that mimic common conditions.
Key biases that affect the clinical decision making process include:
- Anchoring bias. You fix on the first diagnosis suggested and underweight subsequent evidence that contradicts it.
- Availability bias. You overestimate the probability of diagnoses you have seen recently, regardless of base rates.
- Framing bias. The way a referral note or triage label frames a patient shapes your hypothesis before you examine them.
- Confirmation bias. You seek tests that confirm your working diagnosis rather than tests that could disprove it.
Recognizing these biases is the first step. The practical fix is structured reflection: after forming a working diagnosis, explicitly ask what findings would be present if your diagnosis were wrong. Clinical guidelines help here, but they carry their own risk. Rigid adherence to guidelines without individualized judgment can produce technically correct decisions that are wrong for a specific patient. The principles of medical decision making require you to hold both the guideline and the individual simultaneously.
How can clinicians apply decision making principles to improve patient outcomes?
Applying the principles of medical decision making in daily practice requires translating cognitive frameworks into concrete workflow habits. The following comparison shows how two approaches to the same clinical scenario produce different outcomes.
| Approach | Method | Outcome |
|---|---|---|
| Intuitive only | Pattern match, treat immediately | Fast but misses atypical presentations |
| Analytical only | Full Bayesian workup every time | Thorough but inefficient for routine cases |
| Combined (recommended) | Pattern recognition triggers hypothesis, thresholds guide testing | Accurate and time-efficient |
The combined approach reflects how clinical thresholds work in practice. A patient presenting with classic chest pain and multiple risk factors crosses the treatment threshold for acute coronary syndrome before a troponin result returns. You act. A patient with atypical symptoms and a single risk factor sits below the testing threshold for invasive workup. You observe and reassess.
Documenting your decision rationale is as important as making the right decision. When you record why you ordered a test, what probability estimate drove that choice, and what the patient understood about the risks, you create a clinical record that supports continuity of care. It also supports accurate coding of medical decision making complexity, which directly affects reimbursement for your practice.
RADV audit risk increases when documentation does not reflect the complexity of the clinical reasoning that actually occurred. The decision and the documentation must match.
Pro Tip: After each complex encounter, write one sentence in the chart that captures your reasoning: "Probability of PE estimated low based on Wells score; D-dimer ordered to exclude." That sentence protects you clinically, legally, and financially.
Doctors must assist patients in weighing disease and treatment risks when outcomes are not clear-cut. That explicit conversation, documented in the record, is both good medicine and good compliance practice.
Key Takeaways
Effective medical decision making requires combining pattern recognition with analytical reasoning, integrating patient values through shared decision making, and documenting clinical rationale to support both care quality and accurate reimbursement.
| Point | Details |
|---|---|
| Define the process clearly | Medical decision making integrates clinical data, probability, and patient values to reach diagnostic and treatment choices. |
| Use clinical thresholds | Testing and treatment thresholds prevent unnecessary interventions and missed diagnoses in daily practice. |
| Apply shared decision making | Structured models like team talk, options talk, decision talk complete patient collaboration in about 2.5 minutes. |
| Recognize cognitive biases | Premature closure and anchoring bias are the leading causes of diagnostic error; structured reflection counters both. |
| Document decision rationale | Recording your clinical reasoning supports care continuity, accurate coding, and compliance with audit requirements. |
Why documentation is the part of clinical decision making most practices get wrong
Teaching clinical reasoning in medical school has improved significantly over the past decade. Programs now explicitly address Bayesian thinking, shared decision making frameworks, and cognitive bias. What training still underemphasizes is the translation of that reasoning into documentation.
I have reviewed hundreds of clinical records where the physician clearly made a sophisticated, well-reasoned decision. The chart showed none of it. The note read "chest pain, EKG ordered" with no probability estimate, no risk stratification, no record of the patient conversation. That gap costs practices real money through downcoded visits, and it creates audit exposure when payers question whether the level of service billed reflects the complexity of care delivered.
The uncomfortable truth is that shared decision making, Bayesian reasoning, and clinical threshold analysis are only as valuable as your ability to capture them in the record. A decision that is not documented did not happen, at least not in any way a payer or auditor can verify. The future of clinical decision making education needs to close this loop. Teaching the cognitive process without teaching documentation is like teaching surgery without teaching wound closure.
— Elena
How Himshield helps practices protect revenue from documentation gaps
Independent physician practices lose significant reimbursement when the complexity of medical decision making is not captured accurately in the clinical record. Himshield scans your documentation for coding and charge-capture risks before they become denials or audits.
When your clinical reasoning is sophisticated but your documentation is thin, Himshield identifies the gap and gives you physician-friendly guidance to fix it. The platform detects risks tied to medical decision making complexity, HCC gaps, and charge capture errors that most practices never see until a denial arrives. Recover hidden practice revenue and keep every dollar your clinical work has already earned.
FAQ
What is the medical decision making definition?
Medical decision making is the cognitive and analytical process clinicians use to integrate clinical data, patient values, and probability estimates to reach diagnostic and treatment decisions. The Society for Medical Decision Making defines it as a formal discipline drawing on decision psychology, health economics, and clinical epidemiology.
What is the difference between intuitive and analytical decision making?
Intuitive decision making uses pattern recognition for speed and efficiency in clear-cut cases. Analytical decision making applies Bayesian reasoning and clinical guidelines to confirm diagnoses and exclude mimics in complex or ambiguous presentations.
How long does shared decision making take in practice?
Structured shared decision making models like team talk, options talk, decision talk can be completed in about 2.5 minutes. The process does not require full consensus, only patient understanding and alignment with personal values.
What is premature closure in clinical decision making?
Premature closure is the cognitive bias where a clinician stops considering alternative diagnoses once a plausible explanation appears. It is one of the most common causes of diagnostic error and is countered by deliberately asking what findings would be present if the working diagnosis were wrong.
Why does documenting medical decision making complexity matter for reimbursement?
Accurate documentation of clinical reasoning, including probability estimates, risk-benefit discussions, and patient conversations, determines the complexity level coded for a visit. Underdocumented encounters are frequently downcoded by payers, reducing reimbursement for work already performed.