A Risk Adjustment Data Validation (RADV) audit is the official CMS procedure that verifies Medicare Advantage payments accurately reflect each enrollee’s clinical risk by confirming submitted diagnosis codes are supported in the medical record. For independent physician practices, the RADV audit process explained here is not abstract policy. It directly affects your revenue, your compliance standing, and your exposure to federal scrutiny. CMS has expanded audit frequency and updated documentation standards in 2026, making it critical for administrators and compliance officers to understand every stage of this process before a notification letter arrives.
How does the RADV audit process work step by step?
The RADV audit process follows a defined sequence from CMS contract selection through final result reporting. Understanding each stage gives your practice the lead time to respond without scrambling.
Step 1: Contract Selection and Notification

CMS selects Medicare Advantage Organizations (MAOs) for audit based on payment year samples, with a focus on enrollees in the top quartile of risk scores. CMS transitioned to annual, recurring RADV audits starting with Payment Year 2020. For the current cycle, CMS notified contracts on march 20, 2026. That notification is your official start clock.
Step 2: Sample Size Determination
Sample sizes range from 35 to 200 enrollees depending on contract size. Each sampled enrollee has specific Hierarchical Condition Categories (HCCs) flagged for review. Your practice may receive a request for records tied to one or several of those enrollees.
Step 3: Medical Record Submission Window
The submission window for PY 2020 runs from april 13 through august 28, 2026. Records must be submitted through the CMS RADV Web Portal. Only face-to-face encounter documentation from the data collection year qualifies. Submitting the wrong record type or missing the deadline creates immediate risk.
Step 4: CMS Review and Diagnosis Validation
CMS auditors review each submitted record against the MEAT criteria (Monitor, Evaluate, Assess, Treat) to confirm the diagnosis was actively addressed during the encounter. Auditors also verify provider type, signature, and date of service. Records that fail any of these checks result in an HCC being invalidated.
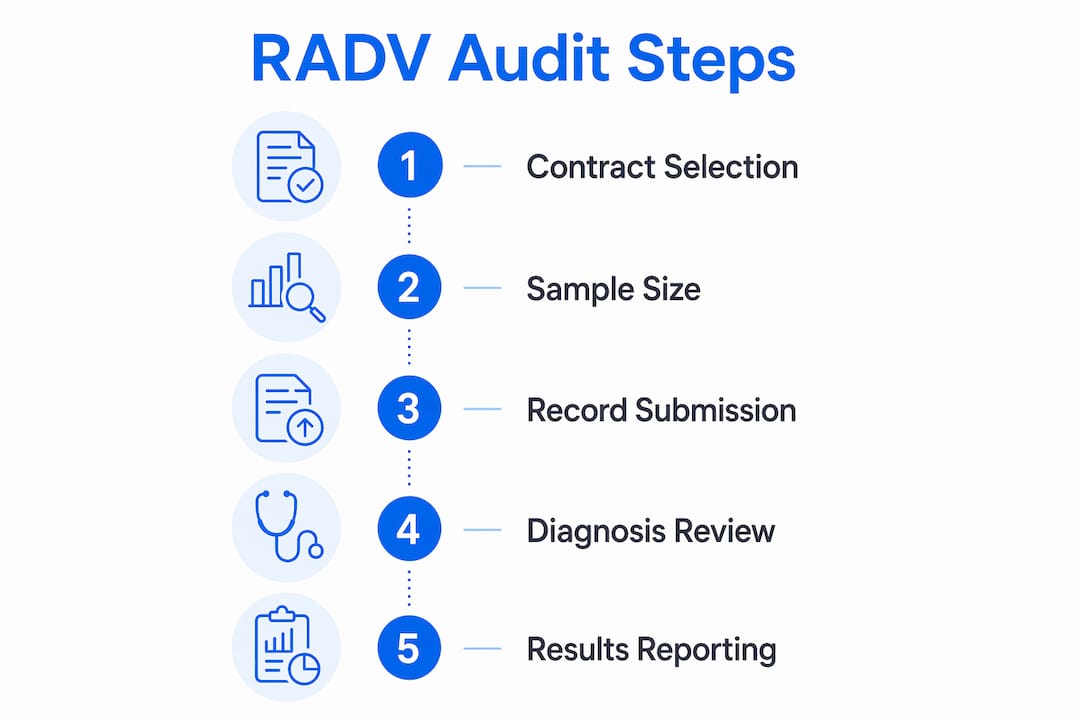
Step 5: Result Reporting and Reconsideration
CMS issues audit findings to the MAO. If diagnoses are invalidated, the MAO faces payment recovery. MAOs retain reconsideration rights to dispute findings with additional documentation. Your practice should be prepared to support that reconsideration process with complete, organized records.
Pro Tip: Request copies of all records submitted on your behalf by the MAO before the submission window closes. Gaps you catch early are far easier to address than discrepancies discovered after CMS issues findings.
What documentation standards must be met to pass a RADV audit?
The MEAT standard is the single most important documentation framework in any RADV audit overview. Every audited diagnosis must show evidence that the provider actively managed the condition during a qualifying encounter.
What MEAT Requires in Practice
-
Monitor: The provider documents signs, symptoms, or test results related to the condition.
-
Evaluate: The note reflects assessment of the condition’s status or response to treatment.
-
Assess: The provider makes a clinical judgment about the condition, including its current severity or stability.
-
Treat: The note documents a management decision, such as medication adjustment, referral, or continued therapy.
A single face-to-face encounter note that satisfies any one of these four elements is sufficient to validate the diagnosis. Only one valid medical record per audited HCC is needed to confirm support, though submitting two records adds a safety margin.
What Does Not Count
CMS requires diagnoses to be documented on the date of service during a qualifying face-to-face visit with an acceptable provider type. Lab reports, radiology results, and pharmacy records do not satisfy MEAT on their own. Problem lists carried forward from prior years without active clinical engagement during the encounter also fail. This is one of the most common and costly misunderstandings in independent practices.
Acceptable provider types include physicians, nurse practitioners, physician assistants, and clinical nurse specialists, provided they are operating within their licensed scope. The provider’s legible signature or electronic authentication must appear on the record.
Pro Tip: Review your EHR templates for chronic condition documentation. If your template auto-populates a problem list without prompting the provider to add MEAT-compliant language, that template is a liability in a RADV audit.
What recent changes affect RADV audits in 2026?
The 2026 audit cycle brings several updates that change the risk profile for independent physician practices. The table below summarizes the most consequential shifts.
| Change | Detail | Impact on Practices |
|---|---|---|
| Annual recurring audits | CMS moved from periodic to yearly RADV cycles starting PY 2020 | Practices face continuous audit exposure, not one-time events |
| CMS-HCC v28 mapping | Updated ICD-10 to HCC crosswalks fully implemented in 2026 | Codes valid under v24 may no longer map to an HCC under v28 |
| Extrapolation status | Legal challenges vacated the 2023 final rule on contract-level extrapolation | Financial exposure remains uncertain but potentially significant |
| Hardship exceptions | Hardship exemption deadline for PY 2020 is september 11, 2026 | Approval is not guaranteed; practices should not rely on this option |
| Legal escalation risk | Patterns of clinical inaccuracy may trigger federal scrutiny beyond payment recovery | Documentation errors can become False Claims Act exposure |
The CMS-HCC v28 update deserves particular attention. Practices using outdated ICD-10 to HCC crosswalks risk submitting risk scores that no longer align with current CMS mapping. That mismatch can invalidate HCCs that would have been valid under the prior model. Verify that your coding team and any billing software you use have been updated to reflect v28.
The extrapolation question also remains unresolved. CMS is conducting audits that could support contract-level extrapolation, meaning a small sample of invalidated diagnoses could be projected across an entire contract population. The financial stakes of that outcome are substantial, even though no final rule is currently in effect.
How can independent practices reduce RADV audit risk?
Preparation for a RADV audit is not a one-time project. It requires building documentation habits that hold up under CMS review every single day.
-
Conduct internal pre-audit reviews. Self-reviews simulating CMS RADV auditors identify systemic documentation errors before an official audit occurs. Pull random charts quarterly and evaluate them against current ICD-10-CM mappings and MEAT criteria.
-
Stop relying on problem lists. Practice notes relying on carry-forwarded chronic condition lists without active MEAT documentation are a frequent cause of RADV denials. Train providers to document active management, not just list conditions.
-
Verify provider credentials and signatures. Every audited record must show an acceptable provider type with a legible, dated signature or electronic authentication. Missing or illegible signatures are an easy fix that practices often overlook until it is too late.
-
Update your ICD-10 to HCC crosswalks. With CMS-HCC v28 fully in effect, any coding tool or reference guide still running on v24 mappings will generate errors. Audit your technology stack now.
-
Document coding rationale explicitly. When a provider assigns a complex or high-weight HCC code, the note should make the clinical basis obvious to an outside reviewer. Specificity in documentation protects the code.
-
Build a RADV audit checklist. A written checklist covering provider type, MEAT elements, date of service, signature, and diagnosis specificity gives your team a repeatable standard for every encounter.
Key takeaways
A successful RADV audit defense depends on MEAT-compliant documentation, current ICD-10-CM v28 mappings, and proactive internal review before CMS notification arrives.
| Point | Details |
|---|---|
| MEAT criteria is non-negotiable | Every audited diagnosis must show Monitor, Evaluate, Assess, or Treat evidence in a face-to-face encounter note. |
| Annual audits require year-round readiness | CMS now conducts recurring RADV audits, so documentation standards must be consistent, not just pre-audit. |
| v28 mapping changes risk scores | Outdated ICD-10 to HCC crosswalks can invalidate HCCs that were previously valid under the v24 model. |
| Problem lists alone cause denials | Carry-forwarded chronic condition entries without active clinical engagement fail RADV documentation review. |
| Legal risk exceeds payment recovery | Patterns of inaccurate diagnosis documentation can escalate to federal False Claims Act scrutiny. |
What i’ve learned watching practices get caught off guard
Independent practices consistently underestimate how specific CMS documentation requirements actually are. The MEAT standard sounds straightforward until you pull 50 charts and realize that 30% of them document a chronic condition only on the problem list, with no corresponding clinical narrative in the encounter note. That is not a coding error. It is a documentation culture problem, and it takes months to correct.
The v28 mapping update is the issue I am most concerned about right now. Practices that have not audited their ICD-10 crosswalks since 2024 are likely submitting codes that no longer carry HCC weight. They will not know until CMS invalidates the diagnosis and the MAO comes back for a payment adjustment.
The legal escalation angle also gets too little attention. Most compliance officers focus on the financial recovery risk, which is real. But documentation errors that rise to knowing misrepresentation can draw False Claims Act scrutiny. That is a different category of problem entirely, and it is one that no independent practice is equipped to handle without significant legal support.
My honest advice: treat every annual wellness visit and chronic care management encounter as if a CMS auditor will read it tomorrow. That standard, applied consistently, eliminates most RADV risk before it starts.
— Elena
How Himshield helps practices stay radv-ready
Independent physician practices do not have the compliance infrastructure that large health systems use to prepare for RADV audits. Himshield was built specifically for that gap.
Himshield scans your coding, documentation, and charge-capture data to identify risks before they become denials or audit findings. The platform flags HCC gaps, detects MEAT documentation deficiencies, and quantifies at-risk reimbursement so you know exactly where your exposure sits. Practices using Himshield recover $5K–$50K+ in hidden revenue while building the documentation defense that RADV audits demand. If you want to see where your practice stands before CMS does, start with a risk assessment from Himshield today.
FAQ
What is a RADV audit?
A RADV audit is a CMS review process that verifies Medicare Advantage diagnosis codes submitted by health plans are supported by clinical documentation in the medical record. The goal is to confirm that risk-adjusted payments accurately reflect each enrollee’s health status.
What does MEAT stand for in RADV audits?
MEAT stands for Monitor, Evaluate, Assess, and Treat. At least one of these elements must appear in a face-to-face encounter note to validate a diagnosis during a RADV review.
How long is the medical record submission window?
For Payment Year 2020, the submission window runs april 13 through august 28, 2026. Missing this window without an approved hardship exception results in the records being excluded from review.
Can a problem list entry satisfy RADV documentation requirements?
No. Problem list entries alone do not meet RADV standards. CMS requires active clinical engagement with the condition during a qualifying face-to-face encounter on the date of service.
What happens if my practice has repeated documentation errors?
Repeated patterns of inaccurate diagnosis documentation can escalate beyond payment recovery. Legal and compliance experts note that patterns of knowing misrepresentation may trigger federal investigations under the False Claims Act.
Recommended
Article generated by HIMShield.